Keywords: Intracellular Calcium, cardiac myocytes, dysregulation, atrial fibrillation
Abstract
Calcium ions are responsible for contraction of muscle throughout the body. Therefore, influx of calcium ions (Ca2+) into atrial myocyte cytoplasm is crucial for the contraction of myocytes during systole. Dysregulation of calcium cycling through sarcoplasmic reticulum (SR) leak and increased activity of the sodium calcium exchanger (NCX). Ultimately leading to transient Ca2+ alternans resulting in delayed afterdepolarisations (DADs) causing overall atrial arrhythmia and fibrillation. Paroxysmal atrial fibrillation (AF) causes substrate remodelling, sustaining and promoting progression to persistent AF.
Calcium cycling mechanisms are therefore a target for antiarrhythmic drugs, although ablation is a more effective but more invasive treatment.
Highlights
- Calcium alternans lead to arrhythmogenesis by being the underlying cause of cardiac alternans
- Dysregulation of intracellular calcium is a complicated process in which CaMKII plays a crucial role in controlling dysregulation
- Intracellular calcium dysregulation can occur during calcium influx to the cardiac myocytes, release from and uptake into the sarcoplasmic reticulum or efflux from the cardiac myocytes
- Understanding dysregulation mechanisms allows for the developments of targeted treatments
- Ablation therapy is still, perhaps, the most effective treatment for atrial fibrillation currently
Clinician’s corner
- All new advancements in understanding causes of intracellular calcium dysregulation and then how this dysregulation causes calcium alternans leading to atrial fibrillation or critical for diagnostic and treatment purposes.
- Recent research has identified new mechanisms that control intracellular calcium dysregulation such as CaMKII and PP1. Animal models have allowed for the development of sarcoplasmic reticulum leak and how CaMKII and PP1 affect the calcium release and uptake from the sarcoplasmic reticulum.
- Understanding initiating mechanisms of atrial fibrillation may also provide a better understanding of the progression of atrial fibrillation and provide methods of halting the progression and development of comorbidities.
- This new knowledge should provide inspiration for research into new anti-arrhythmic drugs to allow for more non-invasive treatment of atrial fibrillation compared to current ablation methods.
Introduction: Understanding Calcium cycling
Ca2+ play an integral role in contraction of cardiac muscle during systole (Eisner, Caldwell, Kistamás, & Trafford, 2017). Understanding causes Ca2+ dysregulation in myocytes can help us understand the processes that lead to arrhythmogenesis, particularly atrial fibrillation, and how to diagnose the disorder and implement treatments (Landstrom, Dobrev, & Wehrens, 2017). Atrial fibrillation is a type of arrhythmia where the atria are not contracting in sinus rhythm causing cardiac output as a whole to be diminished.
The full mechanisms leading to arrhythmogenesis are not fully understood (Dobrev & Wehrens, 2017).This is important going forward if we want to diagnose and treat this condition.
Ca2+ cycling is divided into two steps; increasing and decreasing intracellular calcium. If either of these processes do not occur properly then calcium dysregulation can have adverse effects leading to arrhythmogenesis and remodelling of the heart muscle cells that cause atrial fibrillation (AF) to be sustained and progress from paroxysmal to prolonged, causing chronic adverse health effects (Liu et al., 2020).
The role of Calcium in a regular heartbeat
In a healthy person with a regular sinus rhythm heartbeat, calcium cycling is responsible for the contraction of the cardiac myocytes. Figure 1.A. illustrates the processes of intracellular calcium cycling.

Calcium initially enters cells through voltage gated calcium channel proteins (LTCC) in the sarcolemma. This calcium then binds to ryanodine receptors (RyR) in the sarcoplasmic reticulum (SR) which opens the channel protein and causes an influx of calcium into the cytoplasm from the SR. This is called calcium induced calcium release. Calcium then causes cell contraction through the sliding filament theory and, importantly, after cell contraction the calcium is removed from the cytoplasm. The calcium that was released from the SR is taken back into the SR by sarco-endoplasmic reticulum calcium transport ATPase (SERCA) and the calcium that entered the cell through the LTCC is removed by sodium-calcium exchanger (NCX) proteins by allowing three Na+ into the cell for every one Ca2+ out of the cell. This means that there is no net gain or loss of calcium in the cytoplasm across the whole process per heartbeat.
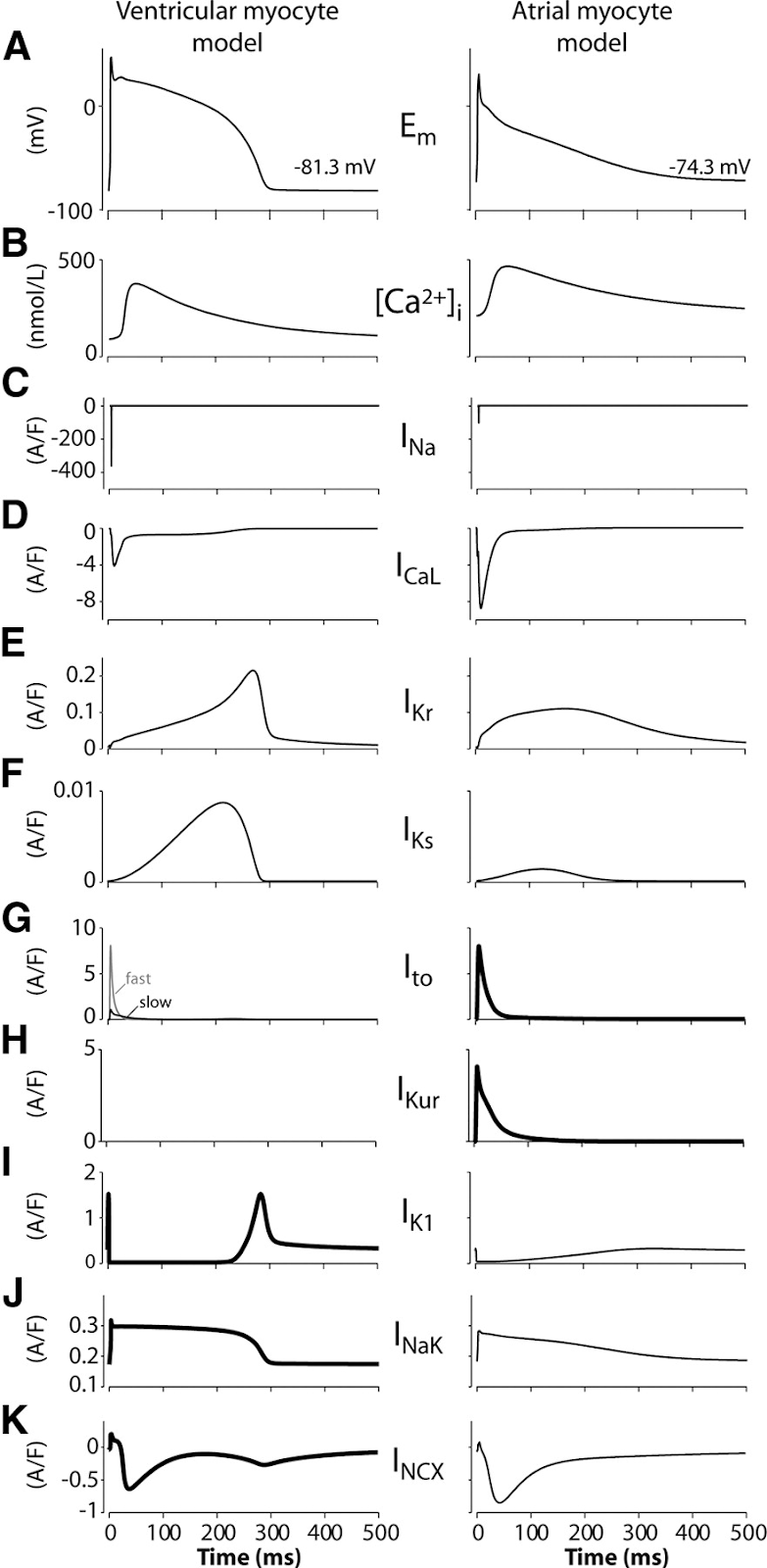
The movement of calcium ions into the cell has an effect on the membrane potential, the voltage across the sarcolemma. The membrane potential is naturally negative and only during systole, when positively charged calcium ions move into the cell through the LTCC, the membrane potential becomes depolarised.The pattern of membrane depolarisation can be seen in Figure 2.A.
In a healthy person this depolarisation only occurs after the action potential from the sino-atrial node opens LTCC to allow calcium to enter the myocyte.
Dysregulation of Calcium cycling leading to arrhythmogenesis
Calcium dysregulation is the underlying cause of cardiac alternans in atrial myocytes (Kanaporis & Blatter, 2015). The indicator of calcium dysregulation is calcium present in the cytoplasm during diastole. Calcium in the cytoplasm can occur in two ways: either calcium is entering the cytoplasm when it shouldn’t be or it is not being removed from the cytoplasm fully after contraction.
CaMKII is a protein that interacts with RyR and this interaction plays a role in arrhythmogenesis as CaMKII phosphorylates RyR to increase the open probability of this channel protein (Heijman, Voigt, Wehrens, & Dobrev, 2014).
The efflux of Ca2+ from the SR through the RyR without the preceding influx of calcium through LTCCs is known as SR calcium leak. The leak of calcium from the SR through the RyR is thought to be a significant contributor to how spontaneous calcium waves may be generated and so has been a subject of study and it has been found that in patients with AF there is enhanced leakage from the SR (Neef et al., 2010; Shan et al., 2012; Voigt et al., 2012; Petrovič, Valent, Cocherová, Pavelková, & Zahradníková, 2015). This indicates that phosphorylation of RyR is an important mechanism in AF and there is evidence that inhibiting CaMKII phosphorylation of RyR may prevent AF (Li et al., 2012). Normally CaMKII phosphorylation of RyR is regulated by protein phosphatase 1 (PP1) to prevent Ca2+ leak and it has been shown that PP1 dysregulation can have the knock-on effect of allowing Ca2+ leak (Chiang et al., 2014; Alsina et al., 2019).
This leak of Ca2+ from the SR causes further calcium induced calcium release in other SRs in the myocyte resulting in an increase in cytoplasmic calcium so when NCX removes this Ca2+, Na+ ions move across the sarcolemma causing depolarisation, independent of the sino-atrial node. Depolarisations caused in this way are called delayed afterdepolarisations (DADs) (Heijman, Voigt, Nattel, & Dobrev, 2014) because they happen after the depolarisation caused by the sino-atrial node. Figure 3 demonstrates one such DAD and how if the depolarisation is large enough, it may trigger an action potential causing LTCC to open simulating a normal action potential. These DADs are linked with AF (Voigt et al., 2012; Heijman, Voigt, Nattel, & Dobrev, 2014; Wit, 2018). Overall this SR Ca2+ leak promotes a substrate for spontaneous AF (Li et al., 2014).
Computational modelling has also shown CaMKII can increase the late Na+ current which has a knock on effect of intracellular Ca2+ accumulation (Onal, Gratz, & Hund, 2017) and additionally in patients with sleep disordered breathing (Lebek et al., 2020).

Ca2+ overloading in the SR is another method that can promote SR Ca2+ leak as this will lead to spontaneous release of Ca2+ without a trigger, known as calcium sparks (Cheng, Lederer, & Cannell, 1993). Overloading of the SR is facilitated by increased SERCA activity (Voigt et al., 2014) and one method for this increased activity could be a lack of sarcolipin (SLN) to regulate SERCA (Xie et al., 2012). Although this is a similar method to generating cardiac alternans in ventricular myocytes, SERCA dysregulation does not cause cardiac alternans in atrial myocytes but does cause Ca2+ alternans (Nassal, Wan, Laurita, & Cutler, 2015). However, research has shown that RyR dysregulation is more important than SERCA dysregulation is regulating Calcium alternans leading to cardiac alternans (Sun et al., 2018).
Overall this dysregulation of Ca2+ may also induce atrial fibrillation by facilitating action potential alternans, in hearts already affected by AF, as well as calcium alternans (Liu et al., 2020). This adds to the belief that “AF begets AF” (Wijffels, Kirchhof, Dorland, & Allessie, 1995) and monitoring the progression of AF from paroxysmal to persistent is important for patient outcomes and potential treatments, as up to >50% of patients may progress to persistent AF within 10 years (Padfield et al., 2017).
Associated conditions and treatments
While AF is a problem in itself, it has some commonly associated diseases; AF is linked with a higher risk of ischemic strokes, even without other risk factors (Go et al., 2018), a potential cause and effect of heart failure (Carlisle, Fudim, DeVore, & Piccini, 2019; Pellicori et al., 2019) and renal failure has a causative link with AF (Huang et al., 2016). Treatment of AF is important in preventing the associated comorbidities and can be dependent on the associated disease, be it heart failure, renal failure or another disease (Szymański, Lip, & Filipiak, 2015).
The most non-invasive form of treatment is by targeted drugs. Since it is established that inhibiting CaMKII can prevent SR Ca2+ leak (Li et al., 2012) then this is a potential target for antiarrhythmics (Mustroph, Neef, & Maier, 2017). Drugs such as Epigallocatechin-3-gallate can act as electrophysiological and Ca2+ homeostatic regulators capable of targeting the atrial myocytes (Chang et al., 2017).
However the focus is shifting towards ablation instead of drugs as ablation techniques are more effective at managing atrial fibrillation, with the greatest success achieved in paroxysmal over persistent (Margulescu & Mont, 2017). Catheter ablation has better patient outcomes with treating AF compared to antiarrhythmic drugs (Poole et al., 2020) and cryoablation has also been shown to be more effective than drugs in a clinical trial (Andrade et al., 2021). Although the efficacy of ablation therapy is still being questioned (Hong, Borges, & Glover, 2020).
The best option should still be to prevent paroxysmal AF from progressing to persistent AF which could be achieved by switching to a healthier lifestyle (Blum et al., 2019).
Concluding remarks
Intracellular calcium dysregulation is the underlying cause of Ca2+ alternans and therefore membrane depolarisation leading to atrial fibrillation. Understanding the mechanisms of this dysregulation allows us to create targeted treatments to mitigate SR leak or inhibited SERCA function.
References
Alsina, K. M., Hulsurkar, M., Brandenburg, S., Kownatzki-Danger, D., Lenz, C., Urlaub, H., … Wehrens, X. H. T. (2019). Loss of Protein Phosphatase 1 Regulatory Subunit PPP1R3A Promotes Atrial Fibrillation. Circulation, 140(8), 681–693. https://doi.org/10.1161/circulationaha.119.039642
Andrade, J. G., Wells, G. A., Deyell, M. W., Bennett, M., Essebag, V., Champagne, J., … Macle, L. (2021). Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation. New England Journal of Medicine, 384(4), 305–315. https://doi.org/10.1056/nejmoa2029980
Blum, S., Aeschbacher, S., Meyre, P., Zwimpfer, L., Reichlin, T., Beer, J. H., … Kühne, M. (2019). Incidence and Predictors of Atrial Fibrillation Progression. Journal of the American Heart Association, 8(20). https://doi.org/10.1161/jaha.119.012554
Carlisle, M. A., Fudim, M., DeVore, A. D., & Piccini, J. P. (2019). Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC: Heart Failure, 7(6), 447–456. https://doi.org/10.1016/j.jchf.2019.03.005
Chang, J.-H., Chang, S.-L., Hong, P.-D., Chen, P.-N., Hsu, C.-H., Lu, Y.-Y., & Chen, Y.-C. (2017). Epigallocatechin-3-gallate modulates arrhythmogenic activity and calcium homeostasis of left atrium. International Journal of Cardiology, 236, 174–180. https://doi.org/10.1016/j.ijcard.2017.01.090
Cheng, H., Lederer, W., & Cannell, M. (1993). Calcium sparks: elementary events underlying excitation-contraction coupling in heart muscle. Science, 262(5134), 740–744. https://doi.org/10.1126/science.8235594
Chiang, D. Y., Li, N., Wang, Q., Alsina, K. M., Quick, A. P., Reynolds, J. O., … Wehrens, X. H. T. (2014). Impaired local regulation of ryanodine receptor type 2 by protein phosphatase 1 promotes atrial fibrillation. Cardiovascular Research, 103(1), 178–187. https://doi.org/10.1093/cvr/cvu123
Denham, N. C., Pearman, C. M., Caldwell, J. L., Madders, G. W. P., Eisner, D. A., Trafford, A. W., & Dibb, K. M. (2018). Calcium in the Pathophysiology of Atrial Fibrillation and Heart Failure. Frontiers in Physiology, 9(). https://doi.org/10.3389/fphys.2018.01380
Dobrev, D., & Wehrens, X. H. T. (2017). Calcium-mediated cellular triggered activity in atrial fibrillation. The Journal of Physiology, 595(12), 4001–4008. https://doi.org/10.1113/jp273048
Eisner, D. A., Caldwell, J. L., Kistamás, K., & Trafford, A. W. (2017). Calcium and Excitation-Contraction Coupling in the Heart. Circulation Research, 121(2), 181–195. https://doi.org/10.1161/CIRCRESAHA.117.310230
Go, A. S., Reynolds, K., Yang, J., Gupta, N., Lenane, J., Sung, S. H., … Solomon, M. D. (2018). Association of Burden of Atrial Fibrillation With Risk of Ischemic Stroke in Adults With Paroxysmal Atrial Fibrillation. JAMA Cardiology, 3(7), 601. https://doi.org/10.1001/jamacardio.2018.1176
Grandi, E., Pandit, S. V., Voigt, N., Workman, A. J., Dobrev, D., Jalife, J., & Bers, D. M. (2011). Human Atrial Action Potential and Ca2+Model. Circulation Research, 109(9), 1055–1066. https://doi.org/10.1161/circresaha.111.253955
Heijman, J., Voigt, N., Nattel, S., & Dobrev, D. (2014). Cellular and Molecular Electrophysiology of Atrial Fibrillation Initiation, Maintenance, and Progression. Circulation Research, 114(9), 1483–1499. https://doi.org/10.1161/circresaha.114.302226
Heijman, J., Voigt, N., Wehrens, X. H. T., & Dobrev, D. (2014). Calcium dysregulation in atrial fibrillation: the role of CaMKII. Frontiers in Pharmacology, 5. https://doi.org/10.3389/fphar.2014.00030
Hong, K. L., Borges, J., & Glover, B. (2020). Catheter ablation for the management of atrial fibrillation: current technical perspectives. Open Heart, 7(1), e001207. https://doi.org/10.1136/openhrt-2019-001207
Huang, S.-Y., Chen, Y.-C., Kao, Y.-H., Hsieh, M.-H., Chen, Y.-A., Chen, W.-P., … Chen, Y.-J. (2016). Renal failure induces atrial arrhythmogenesis from discrepant electrophysiological remodeling and calcium regulation in pulmonary veins, sinoatrial node, and atria. International Journal of Cardiology, 202, 846–857. https://doi.org/10.1016/j.ijcard.2015.10.004
Kanaporis, G., & Blatter, L. A. (2015). The Mechanisms of Calcium Cycling and Action Potential Dynamics in Cardiac Alternans. Circulation Research, 116(5), 846–856. https://doi.org/10.1161/circresaha.116.305404
Landstrom, A. P., Dobrev, D., & Wehrens, X. H. T. (2017). Calcium Signaling and Cardiac Arrhythmias. Circulation Research, 120(12), 1969–1993. https://doi.org/10.1161/circresaha.117.310083
Lebek, S., Pichler, K., Reuthner, K., Trum, M., Tafelmeier, M., Mustroph, J., … Wagner, S. (2020). Enhanced CaMKII-Dependent Late I Na Induces Atrial Pro-Arrhythmic Activity in Patients with Sleep-Disordered Breathing. Circulation Research, 126(5). https://doi.org/10.1161/circresaha.119.315755
Li, N., Chiang, D. Y., Wang, S., Wang, Q., Sun, L., Voigt, N., … Wehrens, X. H. T. (2014). Ryanodine Receptor–Mediated Calcium Leak Drives Progressive Development of an Atrial Fibrillation Substrate in a Transgenic Mouse Model. Circulation, 129(12), 1276–1285. https://doi.org/10.1161/circulationaha.113.006611
Li, N., Wang, T., Wang, W., Cutler, M. J., Wang, Q., Voigt, N., … Wehrens, X. H. T. (2012). Inhibition of CaMKII Phosphorylation of RyR2 Prevents Induction of Atrial Fibrillation in FKBP12.6 Knockout Mice. Circulation Research, 110(3), 465–470. https://doi.org/10.1161/circresaha.111.253229
Liu, T., Xiong, F., Qi, X.-Y., Xiao, J., Villeneuve, L., Abu-Taha, I., … Nattel, S. (2020). Altered calcium handling produces reentry-promoting action potential alternans in atrial fibrillation–remodeled hearts. JCI Insight, 5(8). https://doi.org/10.1172/jci.insight.133754
Margulescu, A. D., & Mont, L. (2017). Persistent atrial fibrillation vs paroxysmal atrial fibrillation: differences in management. Expert Review of Cardiovascular Therapy, 15(8), 601–618. https://doi.org/10.1080/14779072.2017.1355237
Mustroph, J., Neef, S., & Maier, L. S. (2017). CaMKII as a target for arrhythmia suppression. Pharmacology & Therapeutics, 176, 22–31. https://doi.org/10.1016/j.pharmthera.2016.10.006
Nassal, M. M. J., Wan, X., Laurita, K. R., & Cutler, M. J. (2015). Atrial SERCA2a Overexpression Has No Affect on Cardiac Alternans but Promotes Arrhythmogenic SR Ca2+ Triggers. PLOS ONE, 10(9), e0137359. https://doi.org/10.1371/journal.pone.0137359
Neef, S., Dybkova, N., Sossalla, S., Ort, K. R., Fluschnik, N., Neumann, K., … Maier, L. S. (2010). CaMKII-Dependent Diastolic SR Ca2+ Leak and Elevated Diastolic Ca2+ Levels in Right Atrial Myocardium of Patients With Atrial Fibrillation. Circulation Research, 106(6), 1134–1144. https://doi.org/10.1161/circresaha.109.203836
Onal, B., Gratz, D., & Hund, T. J. (2017). Ca2+/calmodulin-dependent kinase II-dependent regulation of atrial myocyte late Na+ current, Ca2+ cycling, and excitability: a mathematical modeling study. American Journal of Physiology-Heart and Circulatory Physiology, 313(6), H1227–H1239. https://doi.org/10.1152/ajpheart.00185.2017
Padfield, G. J., Steinberg, C., Swampillai, J., Qian, H., Connolly, S. J., Dorian, P., … Kerr, C. R. (2017). Progression of paroxysmal to persistent atrial fibrillation: 10-year follow-up in the Canadian Registry of Atrial Fibrillation. Heart Rhythm, 14(6), 801–807. https://doi.org/10.1016/j.hrthm.2017.01.038
Pellicori, P., Urbinati, A., Kaur, K., Zhang, J., Shah, P., Kazmi, S., … Clark, A. L. (2019). Prevalence and Incidence of Atrial Fibrillation in Ambulatory Patients With Heart Failure. The American Journal of Cardiology, 124(10), 1554–1560. https://doi.org/10.1016/j.amjcard.2019.08.018
Petrovič, P., Valent, I., Cocherová, E., Pavelková, J., & Zahradníková, A. (2015). Ryanodine receptor gating controls generation of diastolic calcium waves in cardiac myocytes. The Journal of General Physiology, 145(6), 489–511. https://doi.org/10.1085/jgp.201411281
Poole, J. E., Bahnson, T. D., Monahan, K. H., Johnson, G., Rostami, H., Silverstein, A. P., … Glotzer, T. (2020). Recurrence of Atrial Fibrillation After Catheter Ablation or Antiarrhythmic Drug Therapy in the CABANA Trial. Journal of the American College of Cardiology, 75(25), 3105–3118. https://doi.org/10.1016/j.jacc.2020.04.065
Sedej, S., & Pieske, B. (2012). Mechanisms of Ca2+Triggered Arrhythmias. In T. Yamada (Ed.), Tachycardia (pp. 160–184). https://doi.org/10.5772/25906
Shan, J., Xie, W., Betzenhauser, M., Reiken, S., Chen, B.-X., Wronska, A., & Marks, A. R. (2012). Calcium Leak Through Ryanodine Receptors Leads to Atrial Fibrillation in 3 Mouse Models of Catecholaminergic Polymorphic Ventricular Tachycardia. Circulation Research, 111(6), 708–717. https://doi.org/10.1161/circresaha.112.273342
Sun, B., Wei, J., Zhong, X., Guo, W., Yao, J., Wang, R., … Chen, S. R. W. (2018). The cardiac ryanodine receptor, but not sarcoplasmic reticulum Ca2+-ATPase, is a major determinant of Ca2+ alternans in intact mouse hearts. Journal of Biological Chemistry, 293(35), 13650–13661. https://doi.org/10.1074/jbc.ra118.003760
Szymański, F. M., Lip, G. Y. H., & Filipiak, K. J. (2015). Management of atrial fibrillation in specific patient populations. Kardiologia Polska, 74(1), 1–8. https://doi.org/10.5603/kp.a2015.0223
Voigt, N., Heijman, J., Wang, Q., Chiang, D. Y., Li, N., Karck, M., … Dobrev, D. (2014). Cellular and Molecular Mechanisms of Atrial Arrhythmogenesis in Patients With Paroxysmal Atrial Fibrillation. Circulation, 129(2), 145–156. https://doi.org/10.1161/circulationaha.113.006641
Voigt, N., Li, N., Wang, Q., Wang, W., Trafford, A. W., Abu-Taha, I., … Dobrev, D. (2012). Enhanced Sarcoplasmic Reticulum Ca2+ Leak and Increased Na+ -Ca2+ Exchanger Function Underlie Delayed Afterdepolarizations in Patients With Chronic Atrial Fibrillation. Circulation, 125(17), 2059–2070. https://doi.org/10.1161/circulationaha.111.067306
Wijffels, M. C., Kirchhof, C. J., Dorland, R., & Allessie, M. A. (1995). Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation, 92(7), 1954–1968. https://doi.org/10.1161/01.cir.92.7.1954
Wit, A. L. (2018). Afterdepolarizations and triggered activity as a mechanism for clinical arrhythmias. Pacing and Clinical Electrophysiology, 41(8), 883–896. https://doi.org/10.1111/pace.13419
Xie, L.-H., Shanmugam, M., Park, J. Y., Zhao, Z., Wen, H., Tian, B., … Babu, G. J. (2012). Ablation of sarcolipin results in atrial remodeling. American Journal of Physiology-Cell Physiology, 302(12), C1762–C1771. https://doi.org/10.1152/ajpcell.00425.2011
